STANDARDIZED NATURAL HERBAL THERAPY FOR CHRONIC HEPATITIS B VIRUS (HBV): A COMPREHENSIVE SCIENTIFIC REPORT ON HBV BIOLOGY, MODERN THERAPY LIMITATIONS, cccDNA PERSISTENCE, IMMUNE EXHAUSTION, LIVER INJURY, AND MULTI-TARGET CURATIVE HERBAL STRATEGY
INTRODUCTION: CENTRAL PURPOSE, SCIENTIFIC FOCUS, AND THERAPEUTIC MESSAGE
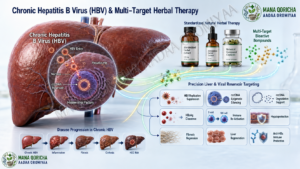
Hepatitis B Virus infection is one of the most serious, complex, and silently progressive viral diseases affecting the human liver. It is not merely a simple infection in which the virus circulates in the blood and can be fully understood by measuring viral load alone. HBV is a biologically advanced hepatotropic DNA virus with the ability to enter liver cells, establish a persistent viral genetic reservoir inside the nucleus of hepatocytes, produce large quantities of viral antigens, manipulate the immune system, exhaust antiviral immune cells, and gradually damage liver tissue without producing obvious early symptoms in many patients. This silent biological behavior makes HBV particularly dangerous because a patient may feel healthy while viral activity, immune dysfunction, inflammation, fibrosis, and liver structural injury are progressing inside the body.
The central message of this report is that Hepatitis B Virus infection, if it has not progressed into advanced hepatocellular carcinoma, should not be viewed as a hopeless or naturally incurable disease. The disease is serious and biologically difficult, but difficulty does not mean impossibility. The major challenge is not that HBV can never be treated at its root; rather, the challenge lies in the limited aim and biological reach of conventional modern antiviral therapy. Modern antiviral drugs are mainly designed to suppress viral replication in the bloodstream, not to fully eliminate the hidden nuclear viral reservoir, restore exhausted immune function, clear HBsAg antigen burden, reverse liver fibrosis, and regenerate damaged liver tissue. Therefore, the limitation is found in the target and objective of the treatment strategy, not in the absolute impossibility of the disease itself.
This report presents a complete scientific explanation of HBV biology, the reasons modern antiviral therapy is mainly a control therapy, the central role of cccDNA in chronic viral persistence, the mechanisms of immune evasion and immune exhaustion, the progression of HBV-related liver damage, and the scientific rationale for standardized natural herbal therapy prepared through the integrative approach of Giddu Gala Yaala Aadaa Oromiyaa. The report explains how properly formulated natural herbal medicines may act through a multi-target therapeutic strategy by reducing viral replication, targeting cccDNA activity, supporting cccDNA degradation, clearing HBsAg, restoring immune function, protecting hepatocytes, reducing fibrosis, supporting cirrhosis remodeling where possible, and promoting liver regeneration. The objective is to present a root-focused, biologically integrated, and scientifically organized model of herbal HBV therapy that goes beyond temporary viral suppression and aims toward durable functional recovery.
This report is written for readers who seek a high-level scientific explanation of the question: “How can standardized natural herbal therapy act against Hepatitis B Virus?” It is intended for health professionals, laboratory personnel, biomedical readers, researchers in traditional medicine, herbal medicine practitioners, and educated patients who want to understand the biological logic behind a multi-target herbal therapeutic system. The discussion is intentionally detailed because HBV itself is not simple. A simplified explanation cannot fully describe the relationship between HBV replication, cccDNA persistence, immune tolerance, HBsAg overload, liver fibrosis, cirrhosis, and liver regeneration. Therefore, this report follows a step-by-step scientific structure from viral biology to therapeutic mechanisms and clinical outcomes.
HEPATITIS B VIRUS AS A SILENT, DANGEROUS, AND BIOLOGICALLY COMPLEX LIVER DISEASE
Hepatitis B Virus infection, commonly known in many communities as a severe liver disease or “Dhibee Simbiraa,” is one of the most dangerous infectious diseases that damages the liver. The virus may enter the body and remain silent for a long period, causing hidden liver injury without clear symptoms. Many patients do not know they are infected until they undergo laboratory testing, blood donation screening, premarital examination, pregnancy screening, or investigation for abnormal liver enzymes. This silent nature is one of the reasons HBV is dangerous. A person may appear healthy while the virus continues to affect hepatocytes, produce viral antigens, alter immune function, and gradually trigger liver inflammation.
The liver is a central organ for metabolism, detoxification, protein synthesis, bile production, hormone regulation, nutrient processing, and immune surveillance. When HBV infects the liver, it does not only create a viral problem; it creates a systemic liver health problem. Chronic HBV can lead to persistent inflammation, oxidative stress, mitochondrial injury, hepatocyte damage, fibrosis, cirrhosis, liver architectural distortion, and, in advanced cases, hepatocellular carcinoma. The disease may move slowly from infection to inflammation, from inflammation to fibrosis, from fibrosis to cirrhosis, and from cirrhosis or chronic viral injury to HCC. Therefore, early and root-focused treatment before advanced cancer development is essential.
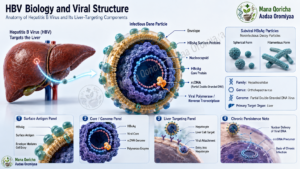
HBV is especially dangerous because it has strong biological mechanisms of hiding. It does not simply remain in the blood. After entering the liver cell, it carries its genetic material into the nucleus of the hepatocyte and establishes a stable viral genetic form known as cccDNA. This nuclear cccDNA acts as a hidden viral factory. While the patient may have no symptoms, this factory can continue to produce viral RNA, viral proteins, HBsAg, HBeAg, and new viral particles. This is why Hepatitis B cannot be understood only by looking at circulating virus in the blood. The real root is inside the liver cell nucleus.
The virus also has the ability to escape the immune system. It produces large quantities of HBsAg and subviral particles that can overwhelm and mislead immune defenses. These particles function as decoys, distracting antibodies and immune cells from the true infected hepatocytes. Over time, the immune system becomes exhausted, especially CD8+ T-cells and natural killer cells. The immune response becomes weak, tolerant, and unable to eliminate the virus effectively. This is why chronic HBV may persist for many years despite the presence of immune cells that would normally fight viral infections.
WHY HEPATITIS B IS COMMONLY BELIEVED TO BE INCURABLE — AND WHY THAT BELIEF IS INCOMPLETE
Many patients become deeply frightened when they are told that they have Hepatitis B. Some patients feel as if their life is approaching its end. This reaction is often caused by the widespread statement that “Hepatitis B has no cure” or “there is no medicine that cures HBV.” Such statements have created fear, hopelessness, and misunderstanding among many patients. However, this belief must be corrected scientifically. The fact that currently available modern antiviral drugs do not usually remove cccDNA does not mean that HBV is naturally impossible to overcome through a deeper multi-target therapeutic approach.
The correct scientific distinction is this: modern nucleoside and nucleotide analogue antiviral drugs mainly reduce HBV replication in the blood, but they do not fully eliminate the hidden root of the virus inside the hepatocyte nucleus. This means the limitation belongs to the mechanism and therapeutic objective of those drugs, not to an absolute biological impossibility of the disease. Saying “modern antiviral drugs are not designed to eradicate cccDNA” is scientifically different from saying “HBV can never be cured.” The first statement is a limitation of a drug class; the second is an incorrect generalization.
Chronic HBV is difficult because the virus hides inside liver cells, maintains cccDNA, produces large amounts of HBsAg, weakens the immune response, induces immune tolerance, and injures liver tissue over time. Therefore, a therapy that aims to overcome HBV must not be limited to viral load suppression. It must address the root viral reservoir, immune dysfunction, antigen burden, and liver damage. If a therapeutic system can reduce viral replication, clear HBsAg, target cccDNA, restore immune function, support anti-HBs formation, and regenerate the liver, then the disease can be approached as an eradicable and recoverable condition before progression to advanced cancer.
MODERN ANTIVIRAL THERAPY: ITS BENEFITS, ITS TARGETS, AND ITS LIMITATIONS
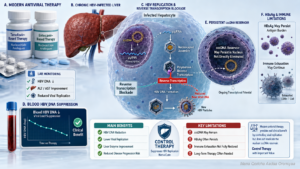
Modern antiviral drugs used for chronic HBV, including Tenofovir formulations such as TDF and TAF, Entecavir, and related nucleoside or nucleotide analogues, have important clinical value. They reduce HBV DNA levels by inhibiting the viral polymerase or reverse transcriptase process. This mechanism blocks the formation of new viral DNA during the replication cycle. As a result, viral load decreases, liver inflammation may improve, ALT and AST may normalize, and progression to cirrhosis or hepatocellular carcinoma may be reduced. These benefits are important and should be recognized.
However, these drugs are primarily viral suppression agents, not complete root-eradication agents. Their main therapeutic objective is to control viral replication in the bloodstream. They are not designed to directly remove cccDNA from the hepatocyte nucleus. They do not fully clear HBsAg antigen burden in most chronic cases. They do not reliably restore exhausted T-cells and NK cells. They do not directly regenerate damaged liver tissue. They do not directly reverse fibrosis and cirrhosis. Their role is to control and stabilize the disease, especially when viral load is high or liver injury has begun.
In many modern clinical approaches, treatment may be started when HBV DNA is high, liver enzymes are elevated, or liver damage is present or likely to develop. Patients with low viral load may be monitored rather than offered a curative intervention. This demonstrates that conventional antiviral therapy is generally structured as disease control, not full disease eradication. It is often given when the virus has already become active enough to threaten the liver. This approach may reduce harm, but it does not necessarily remove the root of infection.
Because modern antiviral drugs do not eliminate cccDNA, many patients must take them for years or for life. When treatment is stopped, the remaining cccDNA reservoir may reactivate and produce new virus. This explains why lifelong therapy is common. The need for long-term therapy does not prove that HBV is naturally incurable. It proves that a treatment focused mainly on reverse transcription and viral load suppression cannot fully address the hidden nuclear reservoir, immune exhaustion, and liver tissue damage.
CONTROL THERAPY VERSUS CURATIVE THERAPY
A clear distinction must be made between control therapy and curative therapy. Control therapy reduces disease activity, slows progression, and helps prevent complications. It is useful, but it does not necessarily remove the root cause. Curative therapy aims to eliminate or permanently neutralize the cause of disease, restore damaged tissue, and create long-term protection. In chronic HBV, modern antivirals are mainly control therapy because they reduce viral replication but do not fully remove cccDNA or restore complete antiviral immunity.
Curative HBV therapy must act beyond viral suppression. It must reduce HBV DNA, clear HBsAg, silence or degrade cccDNA, reactivate exhausted immune cells, support anti-HBs seroconversion, protect hepatocytes, reduce fibrosis, and restore liver function. A therapy that only lowers HBV DNA but leaves HBsAg positive, cccDNA active, immune cells exhausted, and liver tissue damaged cannot be considered complete. A curative system must address the virus and the organ together.
Standardized natural herbal therapy, as presented by Giddu Gala Yaala Aadaa Oromiyaa, is designed as a root-focused curative therapy rather than a simple control therapy. Its purpose is not only to reduce symptoms or lower viral load temporarily, but to address the biological root of the disease, restore immune defense, repair liver injury, and create a sustained recovery pattern. This is the major difference between ordinary viral suppression and a multi-target herbal curative strategy.
THE CENTRAL BIOLOGICAL ROOT: cccDNA INSIDE THE HEPATOCYTE NUCLEUS
The most important biological obstacle in chronic HBV is cccDNA. After HBV enters hepatocytes, the viral genome is transported into the nucleus and converted into covalently closed circular DNA. This cccDNA remains inside the nucleus as a stable viral genetic reservoir. It is not simply a temporary intermediate; it is the central template from which the virus produces viral RNA and viral proteins.
cccDNA behaves like a viral mini-chromosome. It associates with histone proteins and uses host transcription machinery. As long as cccDNA remains transcriptionally active, the virus can continue producing viral RNA, HBsAg, HBeAg, HBcAg, polymerase, and new viral particles. This means that a patient may have reduced virus in the blood but still have the biological root inside the liver.
Modern antiviral drugs mainly block the replication step after viral RNA is already produced. They reduce the production of new viral DNA, but they do not directly destroy the original cccDNA template. Therefore, the viral factory remains. A true curative strategy must reach or influence this hidden reservoir. It must either silence cccDNA, degrade it, prevent its transcription, or support immune-mediated clearance of cells carrying active viral reservoirs.
HBV IMMUNE EVASION, HBsAg DECOYS, AND IMMUNE EXHAUSTION
HBV survives not only by hiding in the nucleus but also by manipulating the immune system. One of its most powerful strategies is the overproduction of HBsAg and subviral particles. These particles may circulate in extremely large quantities. Many of them do not contain complete viral DNA, but they carry surface antigen and occupy the immune system. They act like false targets.
The immune system may spend its energy binding and reacting to these decoy particles while the true infected hepatocytes continue producing virus. This creates immune distraction. Over time, continuous antigen exposure causes immune exhaustion. CD8+ T-cells become weak and less capable of killing infected cells. Natural killer cells lose antiviral strength. Cytokine signaling becomes unbalanced. The body becomes less able to identify and eliminate the true source of infection.
Eventually, chronic HBV may create immune tolerance. In immune tolerance, the body no longer reacts strongly against infected hepatocytes. The virus and host appear to coexist, but this coexistence is harmful. The virus continues producing antigens, and the liver continues experiencing chronic injury. Therefore, a curative therapy must break this immune tolerance safely and restore active antiviral immunity without causing destructive liver inflammation.
LIVER INJURY CAUSED BY CHRONIC HBV
Chronic HBV is not only a viral disease; it is also a progressive liver injury disease. Long-term viral antigen production and immune dysfunction create inflammation inside the liver. Hepatocytes experience oxidative stress, mitochondrial damage, membrane injury, and metabolic imbalance. Liver enzymes may rise as hepatocytes become damaged. Over time, chronic inflammation activates hepatic stellate cells.
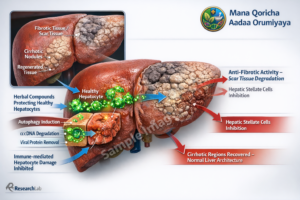
Activated hepatic stellate cells produce collagen and extracellular matrix. This creates fibrosis. Fibrosis is a scar-forming process in the liver. If fibrosis progresses, the liver becomes stiff and distorted. Normal liver architecture becomes replaced by scar tissue and nodular structures. This stage is cirrhosis. Cirrhosis can reduce liver function and increase the risk of liver cancer. Therefore, a successful HBV therapy must not only suppress the virus but also protect and repair the liver.
Patients with chronic HBV may present with different liver morphologies. Some may have enlarged liver size, known as hepatomegaly. Others may have reduced liver size or abnormal liver shape due to advanced fibrosis or cirrhosis. Some may have high viral load but mild liver injury, while others may have lower viral load but significant tissue damage. This variation shows why treatment must be individualized and based on laboratory results, liver imaging, clinical status, and immune condition.
STANDARDIZED NATURAL HERBAL THERAPY: SCIENTIFIC IDENTITY AND THERAPEUTIC PURPOSE
Standardized natural herbal therapy for chronic HBV is not the same as ordinary traditional herbal use. It is a scientifically organized therapeutic system based on selected medicinal plants, standardized botanical extracts, bioactive phytochemical complexes, and structured clinical application. Its foundation includes pharmacognosy, phytochemistry, ethnopharmacology, virology, hepatology, immunology, and patient follow-up.
The purpose of this therapy is to act on HBV at multiple biological levels. It targets viral replication, cccDNA activity, HBsAg antigen burden, immune exhaustion, liver inflammation, oxidative stress, fibrosis, cirrhosis, and hepatocyte regeneration. It is designed to work as a coordinated therapeutic system rather than as one isolated product. Because HBV is complex, the formulation must also be complex in a controlled, standardized, and scientifically organized way.
The formulations may contain bioactive compounds such as flavonoids, alkaloids, terpenoids, polyphenols, curcuminoids, catechins, EGCG, glycosides, antioxidants, hepatoprotective agents, immunomodulators, anti-inflammatory compounds, anti-fibrotic phytochemicals, and regenerative botanical molecules. These compounds work together through synergy. One group may reduce viral replication. Another may regulate immunity. Another may protect liver cells. Another may reduce fibrosis. Another may support liver regeneration. Together, they form a multi-target therapy.
BIOLOGICAL AFFINITY AND HEPATIC DISTRIBUTION OF NATURAL COMPOUNDS
Natural compounds often have biological affinity with human cellular pathways. Many plant-derived molecules can interact with enzymes, receptors, membranes, transporters, antioxidant systems, inflammatory pathways, and immune signaling networks. Since the liver is the central organ of metabolism, orally administered herbal compounds may pass through portal circulation and reach the liver directly through first-pass metabolism. This makes the liver a major target organ for botanical therapy.
For HBV therapy, liver targeting is essential because the virus is established inside hepatocytes. A compound that cannot reach the liver cannot strongly affect HBV. A compound that reaches the liver but cannot enter hepatocytes may also be limited. A compound that enters hepatocytes and influences cytoplasmic and nuclear pathways may have deeper therapeutic potential. Therefore, standardized herbal therapy is built on the idea of hepatic distribution, hepatocyte entry, cellular permeability, and biological activity at the site of disease.
Some natural molecules are small enough to influence intracellular processes. Others modulate signaling pathways indirectly. Some act as antioxidants and reduce oxidative stress. Others regulate immune response. Others may influence epigenetic and transcriptional processes. This multi-level biological compatibility is one reason natural herbal formulations are considered suitable for complex liver diseases such as chronic HBV.
NUCLEAR PERMEABILITY AND TARGETING OF THE HIDDEN VIRAL RESERVOIR
A major limitation of modern antiviral therapy is that the active molecules are not designed to directly destroy cccDNA inside the hepatocyte nucleus. The nuclear pore complex represents a biological barrier. A therapy that cannot influence the nucleus cannot directly address the hidden viral reservoir. Standardized natural herbal therapy is proposed to include small bioactive molecules capable of penetrating hepatocytes and influencing nuclear processes.
The importance of nuclear access cannot be overstated. HBV persistence is not controlled only in the blood. The root is inside the nucleus. Therefore, curative therapy must influence nuclear-level mechanisms such as cccDNA silencing, cccDNA destabilization, HBx inhibition, epigenetic modification, antiviral enzyme activation, and transcriptional shutdown. When herbal compounds influence these processes, they may reduce the ability of cccDNA to function as a viral factory.
This is one of the main scientific explanations for the difference between natural curative therapy and conventional control therapy. Control therapy suppresses the virus after it begins replication. Root-focused therapy aims to stop the viral source itself.
EPIGENETIC SILENCING OF cccDNA: SHUTTING DOWN THE VIRAL FACTORY
The first major mechanism of standardized herbal HBV therapy is epigenetic silencing of cccDNA. cccDNA inside the nucleus is associated with histone proteins and behaves like a viral mini-chromosome. When this structure is open, the virus can produce RNA and proteins. When it is closed, transcription decreases.
Herbal bioactive compounds may influence histone acetylation, histone deacetylation, methylation patterns, chromatin condensation, and transcription factor access. Through these effects, cccDNA may become transcriptionally inactive. Once cccDNA is silenced, viral RNA production decreases. HBsAg production declines. HBeAg and other viral proteins decrease. The viral replication cycle becomes weaker.
This mechanism is essential because it targets the source of viral production. Suppressing HBV DNA in the blood reduces the products of viral replication, but silencing cccDNA reduces the ability of the hidden factory to produce those products. Therefore, epigenetic silencing is a core mechanism in a curative therapeutic model.
HBx INHIBITION AND BLOCKADE OF VIRAL TRANSCRIPTION
HBx is one of the most important viral regulatory proteins in HBV infection. It supports cccDNA transcription, viral persistence, inflammatory signaling, and pathways associated with cancer risk. HBx can be considered a key that helps the virus keep its nuclear factory active. Without HBx support, cccDNA transcription becomes weaker.
Standardized herbal compounds may inhibit HBx-related activity by influencing STAT3, NF-κB, oxidative stress signaling, and inflammatory transcription networks. When HBx signaling is reduced, viral transcription from cccDNA declines. HBsAg production decreases. Viral RNA production becomes weaker. The replication cycle is interrupted at an earlier and deeper level.
Targeting HBx is also important because HBx connects HBV persistence to liver injury and oncogenic risk. By reducing HBx-related signaling, herbal therapy may support both antiviral action and liver protection. This makes HBx inhibition one of the important molecular mechanisms in the proposed therapy.
APOBEC3 ACTIVATION AND DIRECT cccDNA DEGRADATION
A deeper therapeutic goal is not only to silence cccDNA but to promote its degradation. The body has natural antiviral enzymes such as APOBEC3 family enzymes. These enzymes can chemically modify viral DNA, causing damage that leads to fragmentation and degradation. Standardized herbal immunomodulatory compounds may support activation of such endogenous antiviral pathways.
When APOBEC3-like activity is enhanced, viral DNA may undergo cytidine deamination and structural damage. If this process affects cccDNA, the viral reservoir becomes unstable and may be degraded. This is a critical mechanism because it moves beyond suppression and toward removal of the root source.
Silencing cccDNA is like closing the viral factory. Degrading cccDNA is like dismantling the factory itself. A durable curative strategy should support both. When cccDNA activity is shut down and degradation pathways are activated, the possibility of relapse becomes much lower because the source of viral reactivation has been weakened or removed.
SELECTIVE AUTOPHAGY AND LYSOSOMAL VIRAL CLEARANCE
Autophagy is the self-cleaning system of the cell. It allows cells to remove damaged proteins, abnormal structures, dysfunctional organelles, and intracellular pathogens. In the context of HBV, selective autophagy can help remove viral proteins, capsid particles, nucleocapsid materials, and intracellular viral residues. This process may occur through autophagosome formation and lysosomal degradation.
Standardized herbal therapy may support autophagy through AMPK activation, mTOR modulation, mitochondrial protection, lysosomal activation, and reduction of oxidative stress. When autophagy is properly regulated, hepatocytes can clear viral materials without being destroyed. This is known as non-cytolytic clearance.
Non-cytolytic clearance is highly important in HBV because excessive killing of infected hepatocytes may worsen liver inflammation. The ideal therapy should remove the virus while preserving the liver cell. Selective autophagy provides a biological pathway for this balanced action. It helps the cell clean itself from viral materials while maintaining tissue integrity.
IMMUNE RESTORATION AND BREAKING IMMUNE TOLERANCE
A major goal of standardized herbal therapy is immune restoration. Chronic HBV persists because the immune system becomes exhausted and tolerant. T-cells lose antiviral strength. NK cells become weak. Cytokine signaling becomes imbalanced. HBsAg overload distracts immune response. The body stops fighting the virus effectively.
Herbal immunomodulatory compounds may help restore antiviral immunity by reducing antigen burden, improving T-cell function, activating NK cells, supporting Kupffer cell activity, improving antigen presentation, and balancing cytokines. The goal is not uncontrolled immune stimulation. Uncontrolled immune activation may damage the liver. The goal is regulated immune reactivation that allows the body to identify and eliminate HBV while protecting hepatocytes.
When immune tolerance is broken, the body begins to recognize HBV-infected cells again. T-cells and NK cells regain antiviral function. HBsAg clearance becomes possible. Anti-HBs antibody formation becomes possible. This transition from immune tolerance to active antiviral immunity is one of the most important steps toward durable recovery.
HBsAg CLEARANCE AND ANTI-HBs SEROCONVERSION
HBsAg is one of the most important markers and drivers of chronic HBV. High HBsAg burden contributes to immune exhaustion and immune distraction. Therefore, HBsAg clearance is a major milestone in therapy. It indicates that the virus is no longer producing large quantities of surface antigen and that immune pressure is being restored.
Standardized herbal therapy supports HBsAg clearance through several mechanisms. cccDNA silencing reduces HBsAg production. HBx inhibition weakens transcription. Autophagy helps degrade viral proteins. Immune restoration supports antigen clearance from blood. Together, these mechanisms reduce the HBsAg burden and allow the immune system to recover.
Anti-HBs seroconversion is the development of protective antibodies against HBV surface antigen. When a patient becomes HBsAg negative, HBV DNA negative, and anti-HBs positive, this indicates a strong recovery pattern. It means that active viral replication has been suppressed, surface antigen has been cleared, and protective immunity has developed. This is one of the strongest signs of functional recovery.
HEPATOPROTECTION: PROTECTING THE LIVER DURING VIRAL CLEARANCE
A complete therapy for HBV must protect the liver while eliminating the virus. Chronic HBV causes oxidative stress, inflammation, mitochondrial injury, hepatocyte membrane damage, and elevated liver enzymes. If immune restoration occurs without hepatoprotection, liver inflammation may worsen. Therefore, hepatoprotection is an essential component of curative therapy.
Standardized herbal formulations contain antioxidant, anti-inflammatory, and hepatoprotective compounds. These compounds reduce reactive oxygen species, protect mitochondria, stabilize hepatocyte membranes, support glutathione pathways, reduce inflammatory signaling, and protect liver cells from immune-mediated damage. This allows viral clearance to occur in a safer biological environment.
Hepatoprotection is one of the reasons this therapy is broader than ordinary antiviral suppression. The goal is not only to fight the virus but also to protect the organ that has been damaged by the virus. Without liver protection, viral treatment remains incomplete.
FIBROSIS REGRESSION AND CIRRHOSIS REMODELING
Long-term HBV inflammation activates hepatic stellate cells. These cells produce collagen and extracellular matrix, leading to fibrosis. If fibrosis progresses, cirrhosis develops, and liver architecture becomes distorted. Cirrhosis reduces liver function and increases the risk of complications.
Standardized herbal therapy may support fibrosis regression through anti-inflammatory, antioxidant, anti-fibrotic, and regenerative mechanisms. It may reduce hepatic stellate cell activation, lower collagen deposition, support extracellular matrix remodeling, and promote repair of liver tissue. When the fibrogenic process slows down and regeneration improves, liver structure may gradually recover.
In cases where cirrhosis has not progressed to irreversible advanced disease, reducing viral activity, controlling inflammation, and supporting regeneration may improve liver architecture. This is why a root-focused HBV therapy must include anti-fibrotic and liver-regenerative actions.
LIVER REGENERATION AND FUNCTIONAL RESTORATION
The liver has a strong natural capacity for regeneration. However, chronic HBV, inflammation, fibrosis, and oxidative stress can weaken this capacity. Standardized natural therapy supports hepatocyte regeneration by improving mitochondrial function, cellular metabolism, protein synthesis, bile flow, detoxification pathways, and tissue repair signaling.
When hepatocytes recover, liver function improves. ALT and AST normalize as hepatocyte injury declines. ALP and bilirubin normalize as bile flow and detoxification improve. Albumin improves as liver synthetic function returns. Liver size and structure may normalize as inflammation decreases and healthy tissue regenerates. Fibrosis may regress as scar tissue remodeling occurs.
This means that a complete HBV therapy must aim not only for viral negativity but also for liver restoration. A patient should not only become HBV DNA negative; the liver should also return toward normal function and structure.
CLINICAL AND LABORATORY OUTCOMES OBSERVED WITH STANDARDIZED HERBAL THERAPY
According to the clinical observations and internal follow-up experience of Giddu Gala Yaala Aadaa Oromiyaa, patients with chronic HBV who received standardized herbal therapy demonstrated strong improvements across viral, immune, biochemical, and structural liver markers. These patients included individuals with high viral load, HBsAg positivity, abnormal liver enzymes, fibrosis, cirrhosis, abnormal liver size, hepatomegaly, and liver structural changes.
Observed outcomes included HBsAg negativity, HBV DNA PCR becoming undetectable, HBeAg negativity, anti-HBe positivity, anti-HBs positivity above protective levels, normalization of ALT, AST, ALP, bilirubin, and albumin, normalization of liver size, regression or disappearance of fibrosis, absence of detectable cirrhosis, restoration of liver architecture, absence of HBV reactivation, and absence of hepatocellular carcinoma during follow-up.
These outcomes represent recovery at multiple levels. HBsAg negativity indicates antigen seroclearance. HBV DNA negativity indicates suppression of active viral replication. Anti-HBs positivity indicates immune protection. Normal liver function tests indicate biochemical recovery. Restored liver morphology indicates structural recovery. Absence of relapse over years indicates durable clinical stability.
DURABLE FUNCTIONAL RECOVERY AND RELAPSE-FREE FOLLOW-UP
Short-term viral load reduction is not enough to define deep recovery from chronic HBV. A strong therapeutic response must remain stable after treatment. According to the follow-up observations described, patients who achieved HBsAg negativity, HBV DNA negativity, anti-HBs positivity, normal liver function, and restored liver morphology remained stable for years without viral reactivation or biochemical relapse.
This relapse-free pattern indicates durable functional recovery. When the virus does not return, when immune protection remains active, and when the liver remains stable, the response is much stronger than temporary viral suppression. It shows that the therapy has addressed the circulating virus, the antigen burden, the immune dysfunction, and the damaged liver tissue together.
THERAPEUTIC SEQUENCE OF STANDARDIZED HERBAL HBV THERAPY
The therapeutic process follows a step-by-step biological sequence. First, viral replication is suppressed, and HBV DNA decreases. Second, HBsAg antigen burden is reduced, weakening the immune decoy system of the virus. Third, immune exhaustion begins to reverse, allowing T-cells and NK cells to regain antiviral strength. Fourth, cccDNA becomes epigenetically silenced, reducing viral transcription. Fifth, antiviral enzyme pathways and autophagy mechanisms support degradation of viral genetic materials and viral proteins. Sixth, hepatocytes are protected from oxidative and inflammatory damage. Seventh, fibrosis begins to regress as hepatic stellate cell activation decreases. Eighth, hepatocyte regeneration restores liver function and structure. Ninth, anti-HBs immune memory develops, creating long-term protection.
This sequence demonstrates why standardized herbal therapy is designed as a curative model. It does not only suppress the virus. It follows the biological chain required for full recovery: viral suppression, antigen clearance, immune restoration, cccDNA targeting, liver protection, fibrosis regression, liver regeneration, and immune protection.
ACCESSING THE THERAPY
At Giddu Gala Yaala Aadaa Oromiyaa, standardized natural herbal therapy for Hepatitis B is provided as a root-focused curative therapy. The service is designed for patients who want treatment aimed not only at controlling the disease but also at addressing the biological source of the infection and supporting long-term recovery. The treatment plan is based on the patient’s laboratory results, viral markers, liver function, liver status, and general condition.
Patients who cannot come physically may receive therapy where they live, inside or outside the country, based on medical test results and follow-up communication. Patients are advised to complete relevant laboratory and liver investigations, then send clear images or documents of the results through WhatsApp or Telegram. Based on those results, an appropriate treatment protocol can be arranged.
For Hepatitis B and liver disease treatment services, patients can contact the dedicated liver disease center through WhatsApp or Telegram only at:
091 033 3944
Giddu Gala Yaala Dhibee Tiruu Oromiyaa
Mana Qoricha Aadaa Oromiyaa
CONCLUSION
Hepatitis B Virus is not simply a virus in the blood. It is a complex disease involving the hepatocyte nucleus, cccDNA persistence, HBsAg antigen overload, immune exhaustion, immune tolerance, liver inflammation, fibrosis, cirrhosis, and impaired liver regeneration. Modern antiviral drugs can suppress viral replication, but they are not designed to fully remove the hidden viral reservoir, restore complete immune function, clear HBsAg, or regenerate damaged liver tissue.
Standardized natural herbal therapy, as developed and applied through the integrative approach of Giddu Gala Yaala Aadaa Oromiyaa, is designed as a multi-target curative therapy. Its purpose is to reduce viral load, clear HBsAg, target cccDNA, restore immune function, protect hepatocytes, reduce fibrosis, support liver regeneration, and create durable anti-HBs immune protection. By acting on the virus, the immune system, and the liver tissue together, this therapy aims to move beyond disease control and toward complete functional recovery.
Therefore, if Hepatitis B has not progressed to advanced liver cancer, and if treatment is started with proper evaluation, monitoring, and a root-focused therapeutic strategy, recovery is possible. The disease is serious, but it is not hopeless. The key is to use a treatment system that does not only control the virus in the blood, but also addresses the hidden viral reservoir, restores the immune system, repairs the liver, and protects the patient from relapse.